John is a 18 month old boy who comes in today with his parents. He was born full-term and was very healthy until about 6 months ago when he began having frequent ear infections. When he gets an infection, he runs a fever, becomes very fussy, and pulls at his ears. He frequently gets a runny nose and nasal congestion as well. He has been to his pediatrician at least 8 times in the past few months and has taken multiple different antibiotics, including an antibiotic shot at his last visit. Mom says that the antibiotics help with the fevers and ear pain but that the pediatrician always sees “fluid in his ear” at every recent visit. His parents have noticed that he seems to have trouble hearing them at times.
John’s story is a very common one in ENT offices. He has a very classic story for the diagnosis of chronic otitis media. Chronic otitis media (or COM) is defined as fluid trapped behind the eardrum in the middle ear space for at least 3 months. Although this is commonly referred to as a “ear infection,” the fluid behind the eardrum may or may not be infected at any given time.
Regardless of infection status, the fluid in the middle ear typically causes hearing loss. This occurs because the fluid dampens the conduction of sound through the eardrum and ossicles to the inner ear. (You can remind yourself of how the ear works HERE).

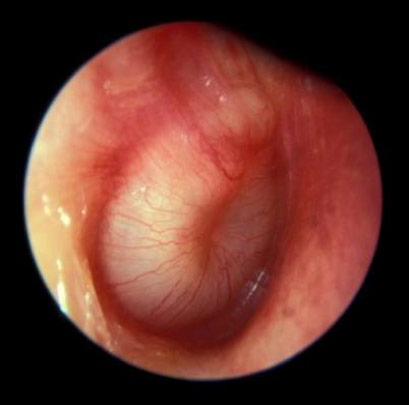
Normal eardrum
Infected fluid seen behind eardrum
If the fluid is present for less than 3 months, doctors usually try treating with medications and waiting for the fluid to clear out. Once it is present for more than 3 months, particularly if frequent infections are happening or if there is documented hearing loss on a hearing test, I recommend placement of ear tubes.
Ear tubes are tiny plastic devices that create a hole through the eardrum. This allows the trapped fluid to drain out into the ear canal and keeps the middle ear space filled with air as it should be.
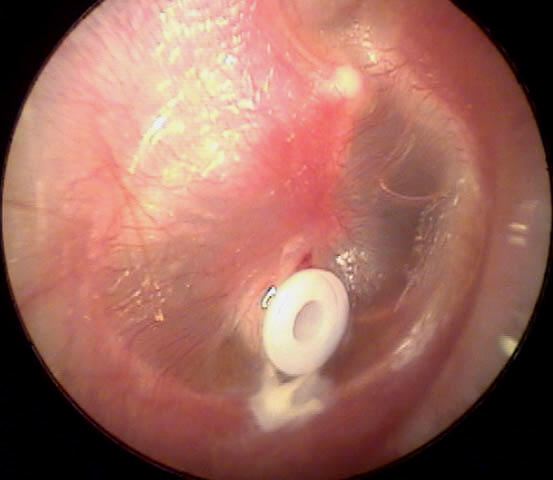
Eardrum with tube in place.
Ear tubes have three main benefits:
1. They improve hearing by removing the fluid behind the eardrum.
2. They reduce or eliminate the typical symptoms of ear infection (pressure, pain, fever).
3. They allow treatment of ear infections with antibiotic drops in the ear instead of antibiotics by mouth.
Ear tubes do not necessarily prevent infections, but they do usually change infections into a much more mild problem that is much easier to treat. However, a lot of patients with tubes do stop having ear infections completely in my experience. I can’t predict ahead of time how any individual will do though.
For children, placement of ear tubes takes me under 10 minutes usually and requires general anesthesia (almost always without any IV necessary). Adults can have the tubes placed in the office (the procedure is less common in adults though).
The procedure is very safe. The main risks are failure to correct hearing loss (uncommon) or having a persistent hole through the eardrum after the tube falls out. There is a miniscule risk of problems due to anesthesia.
After the tubes are placed, they usually stay in the eardrums for 1-2 years, then fall out on their own. At this point, the eardrum usually heals closed. About 75% of children will have grown out of their ear problems after 1 set of tubes. 25% will have recurrence of ear infections and will need another set of tubes put in.